
Are incremental exercise relationships between rating of perceived exertion and oxygen uptake or heart rate reserve valid during steady-state exercises?
- Published
- Accepted
- Received
- Academic Editor
- Peter Federolf
- Subject Areas
- Anatomy and Physiology, Cardiology, Kinesiology, Sports Medicine
- Keywords
- Aerobic exercise, Aerobic exercise prescription, Heart rate reserve, Oxygen uptake reserve, Rating of perceived exertion
- Copyright
- © 2024 Ferri Marini et al.
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2024. Are incremental exercise relationships between rating of perceived exertion and oxygen uptake or heart rate reserve valid during steady-state exercises? PeerJ 12:e17158 https://doi.org/10.7717/peerj.17158
Abstract
Background
Rating of perceived exertion (RPE) is considered a valid method for prescribing prolonged aerobic steady-state exercise (SSE) intensity due to its association with physiological indicators of exercise intensity, such as oxygen uptake (V̇O2) or heart rate (HR). However, these associations between psychological and physiological indicators of exercise intensity were found during graded exercise tests (GXT) but are currently used to prescribe SSE intensity even though the transferability and validity of the relationships found during GXT to SSE were not investigated. The present study aims to verify whether (a) RPE-HR or RPE-V̇O2 relations found during GXTs are valid during SSEs, and (b) the duration and intensity of SSE affect these relations.
Methods
Eight healthy and physically active males (age 22.6 ± 1.2 years) were enrolled. On the first visit, pre-exercise (during 20 min standing) and maximal (during a GXT) HR and V̇O2 values were measured. Then, on separate days, participants performed 4 SSEs on the treadmill by running at 60% and 80% of the HR reserve (HRR) for 15 and 45 min (random order). Individual linear regressions between GXTs’ RPE (dependent variable) and HRR and V̇O2 reserve (V̇O2R) values (computed as the difference between maximal and pre-exercise values) were used to predict the RPE associated with %HRR (RPEHRR) and %V̇O2R (RPEV̇O2R) during the SSEs. For each relation (RPE-%HRR and RPE-%V̇O2R), a three-way factorial repeated measures ANOVA (α = 0.05) was used to assess if RPE (dependent variable) was affected by exercise modality (i.e., RPE recorded during SSE [RPESSE] or GXT-predicted), duration (i.e., 15 or 45 min), and intensity (i.e., 60% or 80% of HRR).
Results
The differences between RPESSE and GXT-predicted RPE, which were assessed by evaluating the effect of modality and its interactions with SSE intensity and duration, showed no significant differences between RPESSE and RPEHRR. However, when RPESSE was compared with RPEV̇O2R, although modality or its interactions with intensity were not significant, there was a significant (p = 0.020) interaction effect of modality and duration yielding a dissociation between changes of RPESSE and RPEV̇O2R over time. Indeed, RPESSE did not change significantly (p = 0.054) from SSE of 15 min (12.1 ± 2.0) to SSE of 45 min (13.5 ± 2.1), with a mean change of 1.4 ± 1.8, whereas RPEV̇O2R decreased significantly (p = 0.022) from SSE of 15 min (13.7 ± 3.2) to SSE of 45 min (12.4 ± 2.8), with a mean change of −1.3 ± 1.5.
Conclusion
The transferability of the individual relationships between RPE and physiological parameters found during GXT to SSE should not be assumed as shown by the results of this study. Therefore, future studies modelling how the exercise prescription method used (e.g., RPE, HR, or V̇O2) and SSE characteristics (e.g., exercise intensity, duration, or modality) affect the relationships between RPE and physiological parameters are warranted.
Introduction
International organizations (Brown et al., 2013; Haskell et al., 2007; O’Donovan et al., 2010; US Department of Health, 2018; Weggemans et al., 2018) recommend performing structured and individually tailored aerobic exercise to improve or maintain cardiorespiratory fitness (CRF), which is associated with health status. Aerobic exercise benefits depend on how exercise prescription’s variables, represented by the FITT-VP (i.e., frequency, intensity, type, time, volume, and progression) principle, are manipulated (ACSM, 2021). In this respect, exercise intensity is pivotal in exercise prescription and its derived benefits. Indeed, to maximize the benefits deriving from an aerobic exercise program (e.g., improvements in CRF) while minimizing the associated risks, it is recommended to prescribe training intensities within certain ranges of minimum and maximal exercise intensities (ACSM, 2021). The traditional approach utilized for prescribing aerobic exercise intensity has been to use a percentage of maximal oxygen consumption (V̇O2max) or maximal heart rate (HRmax) (Mann, Lamberts & Lambert, 2013). However, previous studies argued that is preferable to prescribe exercise based on reserve values (i.e., the difference between maximal and resting values) to take into account the difference in resting metabolic rate and heart rate (Swain & Leutholtz, 1997; Swain et al., 1998). Although aerobic exercise can be prescribed based on exercise intensity domains (i.e., moderate, heavy, and severe (Iannetta et al., 2020; Whipp, 1996)), which are divided by physiological demarcation points (e.g., maximal metabolic steady-state or critical power and lactate or ventilatory threshold) that provide reliable discrimination of the exercise metabolic stimulus (Iannetta et al., 2020), the recommended methods proposed by international organizations (e.g., ACSM, 2021) for aerobic exercise prescription is still based on fixed percentages of reserve (i.e., heart rate reserve (HRR), oxygen uptake reserve (V̇O2R)) and maximal values (i.e., HRmax, V̇O2max). Although it is still a matter of debate (Brawner, Keteyian & Ehrman, 2002; Ferri Marini et al., 2022a; Ferri Marini et al., 2021b; Hui & Chan, 2006; Pinet et al., 2008; Swain et al., 1998), the exercise prescription modality based on percentages of the reserve values is based on the assumption that, during incremental exercise, %HRR and %V̇O2R have a strong correlation and that their regression line is no different from the identity line (i.e., slope = 1 and intercept = 0) (Brawner, Keteyian & Ehrman, 2002; Byrne & Hills, 2002; Colberg, Swain & Vinik, 2003; Dalleck & Kravitz, 2006; Davenport et al., 2008; Lounana et al., 2007; Swain & Leutholtz, 1997). From a practical standpoint, the utilization of this relationship is appealing because it implies that it is possible to elicit a certain metabolic stimulus, namely %V̇O2R, by exercising at the same percentages of HRR. Additionally, the transferability of the relationships between HRR and V̇O2R from incremental to prolonged exercise is another important component that needs to be addressed, which is still subject to debate (Cunha et al., 2011; Wingo, 2015; Wingo, Ganio & Cureton, 2012a). In this respect, previously published articles have demonstrated that the duration (Ferri Marini et al., 2022a) and intensity (Teso, Colosio & Pogliaghi, 2022) of prolonged exercise affect the relationship between HRR and V̇O2R, showing a dissociation between the two reserves and yield higher %HRR than %V̇O2R in exercise having longer duration and higher intensity.
Over the years, other parameters (e.g., rating of perceived exertion (RPE)) have been proposed to prescribe and monitor aerobic exercise intensity because of their association with physiological markers of exercise intensity (e.g., HR, blood lactate, and V̇O2) (Borg, 1974; Irving et al., 2006; Noble et al., 1983; Robertson et al., 2004; Utter et al., 2004). Indeed, RPE was found to be associated with physiological parameters such as HR and blood lactate concentration, independently of age, gender, medical history, level of physical activity, and exercise modality (Scherr et al., 2013); thus, RPE is considered as a reliable measure to monitor and prescribe aerobic exercise (Borg, 1998; Dunbar et al., 1998; Dunbar et al., 1992; Eston & Williams, 1988; Glass, Knowlton & Becque, 1992; Robertson & Noble, 1997). The American College of Sports Medicine (ACSM) guidelines recommend using two RPE scales: the category scale, also known as the original Borg scale, which rates exercise intensity from 6 to 20, and the category-ratio scale of 0–10, which rates exercise intensity from 0 to 10. In this regard, ACSM guidelines recommend using the 6–20 version scale to prescribe moderate (RPE between 12 and 13) or vigorous (RPE between 14 to 17) aerobic intensities (ACSM, 2021). Perceived exertion scales are considered a tool able to consider both physiological and psychological factors during exercise, representing an excellent exercise effort indicator (Morgan, 1994). However, the relationships between RPE and HR, V̇O2, or blood lactate (Borg, Hassmen & Lagerstrom, 1987; Borg, 1974; Dunbar et al., 1992; Glass, Knowlton & Becque, 1992; Irving et al., 2006; Noble et al., 1983; Robertson et al., 2004; Utter et al., 2004) were found during incremental exercises but are used to prescribe and monitor exercise intensity during prolonged constant-intensity exercises. Additionally, there is a high interindividual variability in the relationship between %HRR and %V̇O2R (Ferri Marini et al., 2023), which makes the use of standardized values for the entire population potentially inaccurate at an individual level. Indeed, ACSM guidelines (ACSM, 2012; ACSM, 2021) point out that the RPE responses across exercise modalities and individuals are not comparable due to the high interindividual variability. Therefore, to better individualize the aerobic exercise prescription, international preeminent organizations (ACSM, 2012; Schoenfeld et al., 2021) recommend that individuals should be familiarized with the use of RPE during an incremental exercise test and that the RPE corresponding to the desired exercise training intensities should be pointed out during the incremental test. However, during prolonged constant-intensity aerobic exercise, acute physiological adaptations (i.e., cardiovascular drift and oxygen uptake slow component), which lead to increases in HR and V̇O2 values over time and a dissociation between HR and V̇O2 values (Zuccarelli et al., 2018), could also alter the RPE relations with HR or V̇O2. Consequently, since RPE-based aerobic exercise prescription relies on relationships between RPE and HR or V̇O2 found during incremental exercises (ACSM, 2012; Schoenfeld et al., 2021), which have not been verified during prolonged exercises, their use during prolonged exercise lacks external validity and could lead to different metabolic stimuli than predicted. Indeed, using subjective methods for determining exercise intensity contains some pitfalls, and it requires prior maximal or submaximal exercise testing to anchor the RPE associated with the desired training intensity (e.g., V̇O2) and the need to translate incremental exercise test responses to steady-state training workloads (Bok, Rakovac & Foster, 2022). Therefore, in order to individualize the training prescription, it is recommended to characterize and understand more deeply the transferability of the relationship between RPE and HRR and V̇O2R.
Finally, although exercise intensity is commonly prescribed using HR (due to the simplicity and low costs of HR monitors), no study assessed how exercise intensity, duration, and their interaction of prolonged aerobic exercise affect the RPE-HR and RPE-V̇O2 relationships when HR is used to prescribe and monitor aerobic exercise intensity. Therefore, to the best of our knowledge, no study investigates whether the RPE-HR and RPE-V̇O2 relationships derived from incremental exercise may be transferable to prolonged constant-intensity exercise; hence, confirming the accuracy of these relationships in prescribing and monitoring prolonged constant-intensity aerobic exercise is warranted. Thus, the results of the present study, which complete those presented in our previous companion article (Ferri Marini et al., 2022a), aim to assess if (a) RPE relationships with physiological parameters (i.e., %HRR and %V̇O2R) derived from incremental exercise can be also applied to prolonged exercise and (b) the duration and intensity of prolonged exercise affect these relations.
Materials & Methods
Only the procedures and analyses essential and relevant to the aims of the current study have been included in this section. The readers are referred to the companion article (Ferri Marini et al., 2022a) of the present article, from which the data used in the present study were collected, for a more comprehensive explanation of the study procedures.
Participants
Eight healthy and physically active male participants between the ages 18 and 35 years (mean ± SD: age 22.6 ± 1.2 years; height 1.83 ± 0.08 m, body mass 73.5 ± 9.9 kg, body mass index 21.9 ± 1.4 kg/m2, body fat percentage 14.8 ± 4.0) who have received medical clearance for maximal exercises were enrolled in the present study. Participants were required to have a minimum of three years of treadmill experience. The recruited participants engaged in aerobic exercise training sessions ranging from three to five times per week with at least 4 h dedicated to moderate or higher aerobic training each week (including a minimum of two hours focused on vigorous intensity). Participants who reported the followings were excluded from the study: use of medications that would change the cardiorespiratory responses to exercise (participants did not use any medications during the study), recent orthopedic or musculoskeletal injuries that could affect performance during testing, or smoking habits or use of similar substances.
The study was compliant with the Declaration of Helsinki and was approved by the University of Urbino Human Research Ethics Committee (approval reference number: VN21-10072019). All participants were informed of the potential risks and inconveniences associated with the testing procedures and gave their written informed consent.
Experimental design
Each participant performed seven testing sessions separated by at least 3 days: the first 3 were preparatory for the next 4 experimental trials (see Fig. 1 for a graphical representation of the experimental design). On the first testing day, pre-exercise and maximal HR and V̇O2 were measured. Then, 2 practice trials were performed to determine the running speed yielding the desired HRR percentages (i.e., 60% and 80% HRR). The 4 experimental trials consisted of running exercises on a treadmill for 15 or 45 min of steady state exercise (SSE) at 60% and 80% of HRR. The order of the practice and experimental trials was randomly assigned to each participant. The testing sessions were performed in a controlled indoor environment (temperature: 19–24 °C; humidity: 40–60%; altitude = 77 m above the sea level; with no fan) at the same time to minimize possible effect of circadian rhythm on HR and V̇O2 values. As explained in detail in the companion article (Ferri Marini et al., 2022a), ingestion of liquids or foods was not allowed during the tests. Additionally, participants were asked to avoid changes in their eating habits, vigorous physical activity, and consumption of alcohol and caffeine the day before and the day of testing. The participants were also told to hydrate and drink plenty of fluids the day before and on the day of the trial, drink 0.5 L of water one hour before the session, and fast at least 3 h before the test. The compliance with the above instructions was assessed through a questionnaire specifically created for this study.
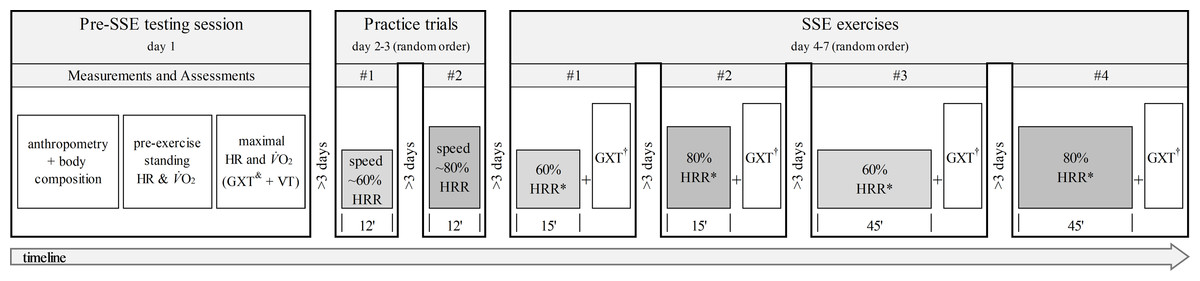
Figure 1: Experimental design and timeline of the non-exercise and exercise (treadmill running at 0% grade) assessments.
SSE, steady-state exercise; HR, heart rate; V̇O2, oxygen uptake; GXT, graded exercise test; VT, verification trial; HRR, heart rate reserve; RPE, rating of perceived exertion; †, GXT performed after SSE with no cessation of exercise or warm-up; &, RPE recorded 15 s before the end of each stage; *, RPE collected at 15 min in the 15-minute SSE and at 45 min in the 45-minute SSE.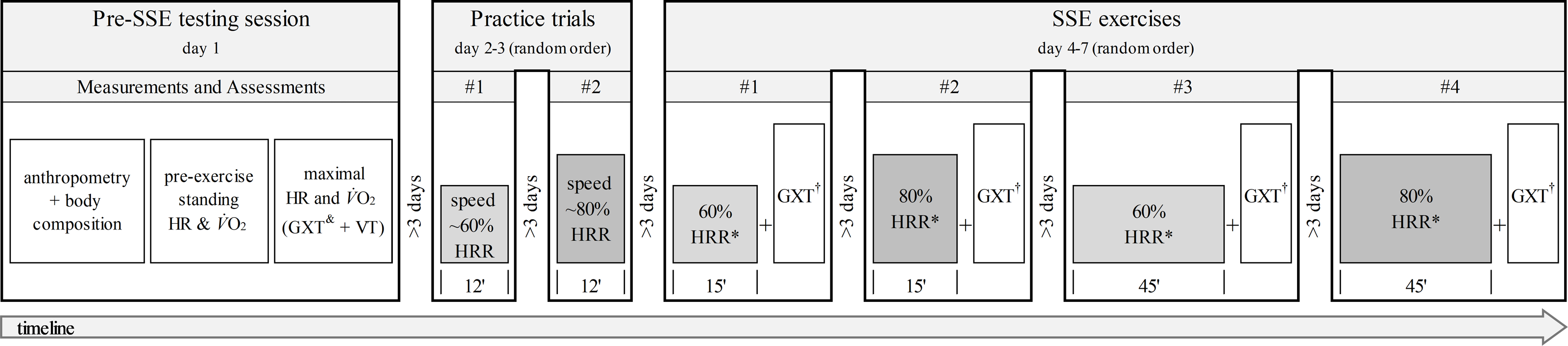{kind=link}
Assessments and data processing
All the exercise tests of this study were performed on the Matrix T7xe treadmill (Johnson Health Tech Italia Spa, Ascoli Piceno, Italy) with 0% slope. In this study, it was not allowed, except for safety reasons, to hold onto the treadmill bars. V̇O2 and HR of the participants were continuously sampled in each testing session. V̇O2, carbon dioxide production, and pulmonary ventilation were monitored and recorded using the portable gas analysis system COSMED K5 (Cosmed, Rome, Italy), which was set up for breath-by-breath data acquisition. Before each test, the system was calibrated using ambient air (21% O2, 0.03 CO2) and a certified gas mixture (16% O2, 5% CO2; Scott Medical Products™, Plumsteadville, USA). The flowmeter turbine was also calibrated using a 3-L syringe according to the instructions of the manufacturer. HR was recorded at heart rate intervals using the Polar V800 HR monitor (Polar Electro Oy, Kempele, Finland).
Anthropometry and body composition
On the first day, the following anthropometric measurements of the participants were taken barefoot and wearing shorts: height (head in the Frankfurt plane), body mass, and body composition (using bioimpedance analysis; BIA 101, Akern-RJL Systems, FI, Italy).
Pre-exercise HR and V̇O2
HR and V̇O2 were recorded continuously for 20 min with the participant standing. The 20 min were divided into four 5-min bins and the first bin was excluded (ACSM, 2021). Then, the bin with the lowest average, for each variable, was considered as pre-exercise HR or V̇O2 (Ferri Marini et al., 2022a).
Maximal exercise test
On the first day, after recording the pre-exercise values of HR and V̇O2, each subject performed 3 min of warm-up at the intensity corresponding to 40% of the maximum estimated speed and immediately performed the control graded exercise test (GXTcont). The GXTcont was created using a personalized ramp protocol designed according to the indication proposed by Da Silva and colleagues (Da Silva et al., 2012), which consisted in persolized increments in treadmill speed according to participants estiatmed V̇O2max every minute till exhaustion. The personalized GXT was created using the spreadsheet provided by Ferri Marini et al. (2021a), which contains detailed information regarding the steps and formulas used for creating the GXT. Briefly, V̇O2max was estimated using the non-exercise model of Matthews et al. (1999). Then, the initial speed of the incremental exercise protocol was set at 50% of the final speed, and the final speed was calculated from the estimated V̇O2max according to the current ACSM equation (ACSM, 2021). The speed was increased every minute by a designated operator. The speed increment value was calculated as the difference between the final and initial speed, which was first divided by 10 min (i.e., the desired test duration), then it was multiplied by the number of minutes passed from the start of the test (excluding warm-up) to the beginning of that stage (e.g., the speeds increment after 1 min of GXT was computed as: (final speed − initial speed)/10 × 1), please see Ferri Marini et al. (2021a) for a detailed explanation of the formulas. This system should allow reaching the final speed and thus the estimated V̇O2max, approximately around the tenth minute of testing (Da Silva et al., 2012). As explained in detail in the companion article (Ferri Marini et al., 2022a), once the GXTcont was completed, participants sat for 20 min (Nolan, Beaven & Dalleck, 2014) after which performed a verification trial (VT). The VT consisted in a warm-up of 2 min at 50% of the maximum speed reached during GXTcont followed by 1 min at 70% of the maximum speed reached during GXTcont. Finally, the treadmill speed was set at 105% of the maximum speed achieved during GXTcont and maintained till exhaustion. The highest V̇O2 and HR, recorded during GXTcont or VT, were considered maximum values if a V̇O2 plateau was present or if the highest HR recorded during GXTcont and VT were within 4 bpm (Midgley & Carroll, 2009). If the data obtained did not meet at least one of these criteria, the test was repeated. During GXTcont and VT, each participant received strong verbal encouragement to make his maximum effort. During GXTcont, the 6–20 RPE values were taken at each stage, 15 s before moving on to the next stage.
Practice trials
Two trials were performed at 60% and 80% of HRR to verify whether the speeds established with the ACSM running equation (ACSM, 2021) would elicit the actual HRR values desired. The practice trials started with 3 min of warm-up at speed corresponding to 40% of V̇O2R; then, the intensity was increased to a speed corresponding to either 60% or 80% of V̇O2R (random order), which, given the 1:1 relationship between %HRR and %V̇O2R, should correspond to 60% and 80% HRR. After 3 min, necessary to reach HRs close to the desired intensity (i.e., 60% and 80% HRR), the speed was adjusted (when needed) every 30s to find the speed yielding the desired target %HRR, which was then used as starting exercise intensity of the SSEs. The practice trials allowed a more accurate determination of the speed yielding the desired HR, which could have been biased by the lack of the 1:1 relationship between %HRR and %V̇O2R (Ferri Marini et al., 2022a; Ferri Marini et al., 2021b; Ferri Marini et al., 2023) or the presence of errors in the ACSM’s running equation. The practice trials were intended to last less than 12 min to avoid possible altered HR responses due to the onset of cardiovascular drift (Wingo, 2015).
Steady-state exercise
After performing the practice trials, each participant performed four SSE trials at different intensities and speeds. All SSEs began with 5 min of warm-up at a speed corresponding to 40% V̇O2R, calculated using the ACSM running equation (ACSM, 2021), followed by 15 or 45 min of run in SSE at 60% or 80% HRR. After the warm-up, the intensity gradually increased every 30 s to reach the starting speed found in the practice trials in 150 s. After about 2 min of running at the starting speed, treadmill belt speed was adjusted to maintain the target HR throughout the SSE session. At the end of the experimental trial, participants immediately (without pause) performed the GXT (GXTpost), already performed on the first day (without the 3-minute warm-up phase) to measure V̇O2peak. The maximal reached values of HR and V̇O2 were used to compute the SSEs’ %HRR-V̇O2R relationships (Wingo, Ganio & Cureton, 2012a). As explained in Ferri Marini et al. (2022a) the testing session was repeated if a steady exercise intensity was not found during the SSE (i.e., the RMSE between the actual and target HR of the trial was higher of 4 bpm) or if either a V̇O2 plateau was not identified during the GXTpost (Midgley & Carroll, 2009) or the highest HR was not within 4 bpm from the HR assumed to be maximal in the pre-SSE session (a total of 3 experimental trials were repeated). During SSE, RPE data (RPESSE) were collected at 15 min in the 15-minute SSE and at 45 min in the 45-minute SSE, using 6–20 scale (Borg, 1998). RPESSE is the actual value of perceived effort at the end of the SSE.
Data preparation and processing
Before the analyses were carried out, dataset preparation, procedure, and data processing were performed. The stationary averages of the last 30-sec of the V̇O2 and HR values recorded for each stage of the GXTcont were computed as a percentage of the reserve values using the following formula: 100 × (recorded value − pre-exercise value) / (maximal value − pre-exercise value). The averages of the last 5 min of the 15- and 45-minute trials were considered as steady-state values of HR and V̇O2, which were converted to percentage values of HRR and V̇O2R (SSE %HRR and SSE %V̇O2R) using pre-exercise data and peaks recorded during the GXTpost following the corresponding SSE. RPE-%HRR and RPE-%V̇O2R relationships obtained during GXTcont were used to estimate RPE values during SSE at 60%HRR and 80%HRR, based on SSE %HRR (RPEHRR) and %V̇O2R (RPEV̇O2R) as follows. First, RPE and %V̇O2R or %HRR paired data points recorded during the GXTcont (warm-up excluded) were used to perform individual linear regressions between RPE and %V̇O2R and RPE and %HRR for each participant using RPE as dependent variable. The regression coefficients (i.e., intercept and slope) and the goodness of fit of the individual linear regressions are shown in Table 1.
Then, participants’ RPEs were predicted using the slopes and the intercepts of the individual linear regression equations between RPE and %HRR or %V̇O2R derived from the GXTcont using the following formulas: slope × SSE %HRR + intercept; slope × SSE % V̇O2R + intercept.
Statistical analysis
The following analyses were used to assess if the individual relationships between RPE-%HRR and RPE-%V̇O2R derived from incremental exercises are different from the relationships found during SSEs of different durations and intensities. Therefore, the RPE predicted from the GXTcont (i.e., RPEV̇O2R and RPEHRR) were separately compared to the RPE recorded during different SSEs (i.e., RPESSE) using two three-way factorial repeated measures ANOVAs. The ANOVAs were performed to assess if the RPE (dependent variable) was affected by the following independent variables: (a) the modality used to determine the RPE (i.e., RPESSE or RPE predicted—modality), (b) the intensity of the SSE (i.e., 60 or 80% of HRR—intensity), and (c) the duration of the SSE (i.e., 15 or 45 min—duration). When a statistically significant result was found, the Bonferroni method was used to perform the post hoc pairwise comparisons. In the present study, three-way factorial repeated measures ANOVAs were used because this comprehensive approach allows a direct assessment of the interaction effect of exercise intensity and duration, which would be neglected if separate two-way ANOVAs for each exercise intensity (assessing modality × duration) or duration (assessing modality × intensity) were performed.
| R | R2 | SEE | Intercept | Slope | |
|---|---|---|---|---|---|
| RPE vs. V̇O2R | |||||
| Mean | 0.944 | 0.893 | 1.122 | −1.370 | 0.209 |
| SD | 0.047 | 0.087 | 0.484 | 4.939 | 0.051 |
| Min | 0.854 | 0.729 | 0.537 | −10.333 | 0.139 |
| Max | 0.988 | 0.976 | 1.872 | 4.599 | 0.286 |
| RPE vs. HRR | |||||
| Mean | 0.965 | 0.930 | 0.929 | −0.482 | 0.194 |
| SD | 0.021 | 0.040 | 0.297 | 3.871 | 0.038 |
| Min | 0.933 | 0.871 | 0.483 | −8.310 | 0.146 |
| Max | 0.993 | 0.986 | 1.311 | 4.603 | 0.260 |
Notes:
- R
-
coefficient of correlation
- R2
-
coefficient of determination
- SEE
-
standard error of estimate
- Intercept
-
intercept of the ILR created during control graded exercise test (GXTcont)
- Slope
-
slope of the ILR created during GXTcont
- RPE vs. V̇O2R
-
ILR between rating of perceived exertion (RPE) and V̇O2R recorded during GXTcont
- RPE vs. HRR
-
ILR between RPE and HRR recorded during GXTcont
- SD
-
standard deviation
Moreover, for each of the four experimental conditions, the Cohen’s d effect size (ES) between RPESSE and RPE predicted was calculated by dividing the mean by the SD of the differences between RPESSE and RPE predicted. Finally, the number of participants whose RPESSE was not within ± 1 of the predicted RPE were computed to assess, on an individual level, the number of overestimation (i.e., difference between RPESSE and predicted RPE lower than -1) and underestimation (i.e., difference between RPESSE and predicted RPE is higher than 1) of the RPESSE. The analyses were performed using SPSS Statistics (IBM, v.20) software, with an α level of 0.05.
Results
Participants’ pre-exercise and maximal HR and V̇O2 values recorded during control tests are: pre-exercise HR = 79.6 ± 10.5 bpm, HRmax = 195.3 ± 11.3 bpm, pre-exercise V̇O2 = 4.6 ± 0.5 mL ⋅min−1 ⋅kg−1, V̇O2max= 61.5 ± 8.6 mL⋅min−1⋅kg−1.
HR and V̇O2 recoded during the SSEs, along with the actual RPE and the RPE predicted according to the GXTcont’s individual linear relationships between RPE and %V̇O2R or %HRR, are reported in Table 2.
| 15 min | 45 min | |||
|---|---|---|---|---|
| SSE at 60% of HRR | SSE at 80% of HRR | SSE at 60% of HRR | SSE at 80% of HRR | |
| HR (bpm) | 150.8 ± 9.7 | 173.4 ± 10.2 | 150.1 ± 9.8 | 173.0 ± 10.5 |
| V̇O2 (mL ⋅ min−1⋅ kg−1 ) | 39.5 ± 6.3 | 52.5 ± 5.5 | 36.4 ± 6.6 | 45.1 ± 4.5 |
| HRpeak (bpm) | 195.2 ± 12.9 | 193.3 ± 10.6 | 190.9 ± 12.0 | 194.5 ± 10.4 |
| V̇O2peak (mL ⋅ min−1⋅ kg−1 ) | 61.7 ± 6.6 | 63.0 ± 6.8 | 58.9 ± 9.4 | 60.7 ± 8.7 |
| RPESSE | 10.6 ± 1.2 | 13.5 ± 1.7 | 12.3 ± 1.7 | 14.8 ± 1.7 |
| RPE V̇O2R | 11.5 ± 2.7 | 15.8 ± 2.1 | 11.0 ± 3.0 | 13.9 ± 1.8 |
| RPEHRR | 11.5 ± 2.1 | 15.5 ± 1.5 | 11.8 ± 2.1 | 15.3 ± 1.5 |
| HRRpeak (%) | 61.7 ± 2.8 | 82.6 ± 1.6 | 63.4 ± 1.5 | 81.4 ± 2.3 |
| V̇O2Rpeak (%) | 60.9 ± 6.7 | 82.1 ± 5.7 | 58.6 ± 7.8 | 72.7 ± 6.4 |
Notes:
- HR
-
heart rate
- V̇O2
-
oxygen uptake
- RPE
-
rating of perceived exertion (6–20)
- SSE
-
steady-state exercise
- HRR
-
heart rate reserve
- V̇O2R
-
oxygen uptake reserve
- SD
-
standard deviation
- HRpeak
-
peak HR recorded during incremental exercises following each SSE
- V̇O2peak
-
peak V̇O2 recorded during incremental exercises following each SSE
- RPESSE
-
rating of perceive exertion recorded during SSE
- RPEV̇O2R
-
rating of perceive exertion predicted from SSE V̇O2R using incremental RPE-V̇O2R relationship
- RPEHRR
-
rating of perceive exertion predicted from SSE HRR using incremental RPE-HRR relationship
The Mean, SD, and ES values of the differences between the RPE values measured during SSE (RPESSE) and the RPEs predicted using the relationship between RPE and V̇O2R (RPEV̇O2R) or HRR (RPEHRR) found during GXTcont are shown in Table 3.
| RPESSE− RPE V̇O2R | RPESSE− RPEHRR | |||
|---|---|---|---|---|
| 15 min | 45 min | 15 min | 45 min | |
| SSE at 60% of HRR | ||||
| Mean | −0.9 | 1.3 | −0.9 | 0.5 |
| SD | 2.8 | 3.2 | 2.1 | 2.3 |
| ES | −0.32 | 0.40 | −0.42 | 0.21 |
| SSE at 80% of HRR | ||||
| Mean | −2.3 | 0.9 | −2.0 | −0.5 |
| SD | 3.2 | 2.7 | 2.2 | 2.2 |
| ES | −0.74 | 0.34 | −0.93 | −0.23 |
Notes:
- SD
-
standard deviation
- ES
-
Cohen’s d effect size
- HRR
-
heart rate reserve
- V̇O2R
-
oxygen uptake reserve
- SSE
-
steady-state exercise
- RPESSE
-
rating of perceived exertion (RPE) reported during SSE
- RPEV̇O2R
-
rating of perceive exertion predicted from SSE V̇O2R using incremental RPE-V̇O2R relationship
- RPEHRR
-
rating of perceive exertion predicted from SSE HRR using incremental RPE-HRR relationship
The number of participants whose RPESSE was not within ± 1 of the predicted RPE, showing, on an individual level, an overestimation or underestimation of the RPESSE are reported in Table 4.
| RPESSE - RPE V̇O2R | RPESSE - RPEHRR | |||
|---|---|---|---|---|
| 15 min | 45 min | 15 min | 45 min | |
| SSE at 60% of HRR | ||||
| Δ <-1 (N) | 3 | 2 | 4 | 3 |
| Δ >1 (N) | 2 | 3 | 1 | 3 |
| SSE at 80% of HRR | ||||
| Δ <-1 (N) | 5 | 2 | 5 | 2 |
| Δ >1 (N) | 1 | 3 | 0 | 2 |
Notes:
- HRR
-
heart rate reserve
- V̇O2R
-
oxygen uptake reserve
- SSE
-
steady-state exercise
- RPESSE
-
rating of perceived exertion (RPE) reported during SSE
- RPEV̇O2R
-
rating of perceive exertion predicted from SSE V̇O2R using incremental RPE-V̇O2R relationship
- RPEHRR
-
rating of perceive exertion predicted from SSE HRR using incremental RPE-HRR relationship
RPESSEvs RPEV̇O2R
Measured and V̇O2R estimated RPEs were affected by intensity (F(1,7) = 68.744, p < 0.001, partial eta-squared () = 0.908), but they were not affected by the modality (F(1,7) = 0.088, p = 0.775, =0.012) and duration (F(1,7) = 0.081, p = 0.784, =0.011).
The interactions between duration × modality (F(1,7) = 9.030, p = 0.020, = 0.563) and duration × intensity (F(1,7) = 6.676, p < 0.036, = 0.488) showed a significant effect on RPE, whereas the interactions between intensity × modality (F(1,7) = 2.394, p = 0.166, = 0.255) and intensity ×duration ×modality (F(1,7) = 4.778, p = 0.065, = 0.406) were not significant.
RPE was higher at higher intensity, with a significant mean difference between 80% of HRR (14.5 ± 2.0) and 60% of HRR (11.3 ± 2.2) of 3.1 ± 1.6, p < 0.001.
When the modalities were compared at different SSE durations, RPESSE did not increase significantly from SSE of 15 min (12.1 ± 2.0) to SSE of 45 min (13.5 ± 2.1), with a mean change of 1.4 ± 1.8, p = 0.054. Whereas RPEV̇O2R decreased significantly from SSE of 15 min (13.7 ± 3.2) to SSE of 45 min (12.4 ± 2.8), with a mean change of −1.3 ± 1.5, p = 0.022.
RPESSEvs RPEHRR
Measured and HRR-estimated RPEs were only affected by intensity (F(1,7) = 79.933, p < 0.001, = 0.919), whereas duration (F(1,7) = 4.744, p = 0.066, = 0.404), modality (F(1,7) = 1.165, p = 0.316, = 0.143), and the interaction between duration × intensity (F(1,7) = 3.117, p = 0.121, = 0.308), duration × modality (F(1,7) = 5.506, p = 0.051, = 0.440), modality × intensity (F(1,7) = 5.089, p = 0.059, = 0.421), and duration × modality × intensity (F(1,7) = 0.256, p = 0.628, = 0.035) did not show a significant effect on RPE.
Discussion
The results of the present study are the first to assess the transferability of the RPE-%HRR and RPE-%V̇O2R relationships from incremental to prolonged exercise prescribed using HR, which is one of the underlying assumptions based upon which world’s preeminent organizations (ACSM, 2012; Schoenfeld et al., 2021) recommend using the RPE-based methods for prescribing aerobic exercise intensity. However, it is worth notice that the results of the present study were collected in a small sample of physically active males, which, as explained in detail at the end of the discussion, limits and reduce the generalizability of the findings. The present study demonstrates that, as expected, exercise intensity affects RPE, with higher exercise intensities yielding higher RPEs during both GXTs and SSEs. This result confirms the presence of a correlation between perceived exertion and exercise intensity, which is the underlying theoretical construct that allows the use of RPE scales for prescribing and monitoring exercise intensity during aerobic (Borg, 1998; Dunbar et al., 1998; Dunbar et al., 1992; Eston & Williams, 1988; Glass, Knowlton & Becque, 1992; Robertson & Noble, 1997) and resistance (Ferri Marini et al., 2022b; Gearhart Jr et al., 2002; Lagally et al., 2004; Lea et al., 2022; Morishita et al., 2018; Pincivero, Coelho & Campy, 2003) exercise. A novel result that can be observed in the present study derives from the comparison of RPEV̇O2R and RPESSE, which shows a significant effect of the interaction between duration and prediction modality used on RPE, yielding a dissociation, over time, between the actual and the V̇O2 predicted RPE. Indeed, from 15 to 45 min SSE, it is noticeable an increase of 1.4 ± 1.8 in RPESSE and a decrease of 1.3 ± 1.5 in RPEV̇O2R, showing an opposite trend with increasing duration. Likewise, the interaction effect between prediction modality based on HRR and duration, even though not reaching a statistical significance, showed a tendency towards a significant effect (p = 0.051), yielding an increase of 1.4 ± 1.8 in RPESSE with no changes in RPEHRR (0.0 ± 0.5).
Additionally, as shown in Table 3, it is possible to notice a tendency showing that intensity may also affect the relationship between RPESSE and RPE V̇O2R or RPEHRR, with higher intensity SSEs (i.e., 80%HRR) showing mean differences (i.e., RPESSEminus RPEV̇O2R or RPEHRR) from −0.4 to −1.4 lower than lower intensity SSE (i.e., 60%HRR) for both RPEV̇O2R and RPEHRR in both 15- and 45-min conditions. Since the mean differences between RPESSE and RPEV̇O2R or RPEHRR tended to be lower at higher intensities, higher SSE intensity caused the incremental exercise relationships between RPE and V̇O2R or HRR to overestimate the actual RPESSE compared to the lower SSE intensity.
The results of the present study (Table 3) point out that also the duration may affect the relationship between RPESSE and RPEV̇O2R or RPEHRR with longer duration SSEs (i.e., 45 min) showing mean differences (i.e., RPESSEminus RPEV̇O2R or RPEHRR) from 1.4 to 3.2 higher than shorter duration SSE (i.e., 15 min) for both RPEV̇O2R and RPEHRR in both 60% and 80% conditions. Since the mean differences between RPESSE and RPE V̇O2R or RPEHRR tended to be higher at longer durations, longer SSE duration caused the incremental exercise relationships between RPE and V̇O2R or HRR to underestimate the actual RPESSE compared to the shorter SSE duration.
When the results of the present study are interpreted on an individual level, assessing the number of participants whose RPESSE was not within ± 1 of the predicted RPE, the effect of SSE duration and intensity seem to be confirmed, showing that the RPESSE was overestimated in more participants, with fewer underestimations, in shorter duration and higher intensity SSEs.
Overall, the above results highlight that when aerobic exercise intensity is prescribed using a fixed %HRR, predicting RPE using RPE-%V̇O2R relationships found during incremental exercise yields inaccurate estimations of the SSE intensity in healthy males, whereas the RPEHRR values do not significantly differ from RPESSE values. However, it is worth noting that both relationships (i.e., RPE-%HRR and RPE-%V̇O2R) seem to be affected by the duration and intensity of prolonged aerobic exercise.
The results of the present study are in line with those found by previous studies aiming at investigating the suitability of RPE as an aerobic exercise intensity prescription method, which found an association between RPE and physiological parameters during incremental exercise (Dunbar et al., 1994; Dunbar et al., 1992; Glass, Knowlton & Becque, 1992). Although similar, the results of the present study partly contrast with those found by Glass and colleagues (Glass, Knowlton & Becque, 1992), who tried to assess if RPE derived from GXT could be used to prescribe SSE intensity based on the RPE-HR relationship and demonstrated that RPE obtained from GXT can accurately prescribe exercise intensity during treadmill running. However, the results of the present study and those from Glass, Knowlton & Becque (1992) are not entirely comparable because of the different durations of the exercises (i.e., 15 and 45 min compared to 10 min used from Glass et al.). In particular, the current study highlights that the relationship found during incremental exercise, when used to prescribe prolonged exercise, could be affected by SSE duration. Therefore, the shorter duration (10 min of exercise) used by Glass, Knowlton & Becque (1992), may not be sufficient to see the physiological adjustment in HR (i.e., cardiovascular drift) that occurs approximately after 10–15 min of moderate-intensity exercise (Wingo, Ganio & Cureton, 2012a).
The results of the present study show that not all the physiological parameters can be used to predict the actual RPE during SSE in healthy males. Specifically, while RPESSE and RPEHRR did not change significantly with longer duration, RPEV̇O2R decreased significantly from shorter to longer SSEs. These results may be due to physiological adjustments present during prolonged exercise, namely the so-called slow components (Jones et al., 2011), which affect both V̇O2 and HR (i.e., cardiovascular drift) influencing the transferability of the relationship between HR and V̇O2 from incremental to prolonged exercise and creating a dissociation between the two parameters during prolonged exercise (Ferri Marini et al., 2022a; Teso, Colosio & Pogliaghi, 2022; Zuccarelli et al., 2018). The results of the present study reinforce all the above and, also, reveal discrepancies between RPE and physiological parameters (i.e., V̇O2R and HRR) when comparing the relationships found during incremental and prolonged exercise, showing that RPESSE is, on average, closer (i.e., smaller differences with predicted RPEs) to RPEHRR compared to RPEV̇O2R.
A novelty of the present study is that, although there are several studies assessing the use of different indicators of exercise intensity (e.g., HR or V̇O2) during prolonged aerobic exercise (see Ferri Marini et al., 2022a), only one (Wingo & Cureton, 2006b) employed prolonged aerobic exercise bouts performed at a constant HR, which is a commonly adopted and recommended practice in aerobic exercise prescription. However, Wingo & Cureton (2006b) did not assess the compliance to the target SSE intensities, whereas in the present study participants’ compliance with the target intensity was assessed by calculating the RMSE between actual and target HR for each subject and SSE condition. Additionally, exercising at constant power output or speed for a prolonged duration yield higher exercise intensity (i.e., HR and V̇O2) due to physiological adjustments like cardiovascular drift and the V̇O2 slow component (Cunha et al., 2011; Teso, Colosio & Pogliaghi, 2022) and lower V̇O2max (Wingo, Ganio & Cureton, 2012a), whereas HRmax has been shown not to be modified by prolonged aerobic exercise (Ganio et al., 2006; Lafrenz et al., 2008; Wingo & Cureton, 2006a; Wingo & Cureton, 2006b; Wingo et al., 2012b; Wingo, Stone & Ng, 2020). Therefore, maintaining a constant HR throughout each condition ensures consistent relative exercise intensity across all SSEs unlike using fixed percentages of V̇O2max or V̇O2R or speeds corresponding to certain V̇O2. During exercise at a fixed %HRR, as proposed in the present study, the discrepancy between RPESSE and RPEV̇O2R may also appear because the work rate (e.g., power output in a cycle ergometer or speed and grade in a treadmill) needs to be reduced as time goes by (Ferri Marini et al., 2022a; Iannetta et al., 2020) to maintain the target HR and avoid the effects of cardiovascular drift yielding lower V̇O2. Indeed, in the current study, as explained in detail in the companion article (Ferri Marini et al., 2022a), treadmill speeds were continuously reduced after reaching target HR to maintain a stable HR during each SSE. The treadmill speeds were decreased of about the same magnitude during the 15-min SSEs at 60% HRR (∼4.3%) and 80% HRR (∼5.7%), whereas a more noticeable decrease in treadmill speeds was observed during the 45-min SSEs at 80% HRR (∼24.1%) compared to SSEs at 60% HRR (∼13.2%). The seemingly higher decrease in treadmill speeds in longer duration and higher intensity SSEs suggests a potential interaction effect between exercise intensity and duration on the cardiovascular drift. Consequently, the one-size-fits-all principle (i.e., the principle of applying a standard method for prescribing exercise without considering interindividual variability in response to prolonged exercise) should be carefully adopted as the aerobic exercise intensity seems to be affected not only by the exercise duration but also by the parameter used to prescribe exercise intensity (e.g., RPE, HR, power output, or V̇O2) in healthy male individuals. Indeed, although in the current study individual RPE-%HRR and RPE-%V̇O2R relationships derived from incremental tests were used, this was not sufficient to accurately predict relationships during prolonged exercise in physically active males. Thus, additional methods able to consider metabolic responses, such as metabolic thresholds (e.g., critical power, maximal metabolic steady state), could increase exercise prescription accuracy (Weatherwax et al., 2019), and further studies investigating whether different methods of prescribing exercise could affect adaptations to exercise are required. Moreover, considering that the RPE predicted by V̇O2R is lower than the actual RPE found during longer SSE, whereas is higher during shorter SSE, using the standardized relationship to transfer the results found in incremental exercise to prolonged exercise could induce individuals to not exercise at the desired intensity. Therefore, an inaccurate prediction of RPE that would lead to a lower intensity than expected may not lead to the desired adaptations from training. On the contrary, prescribing higher intensity than expected could potentially increase the risk associated with exercise due to the higher cardiorespiratory, metabolic, and mechanical stress at higher exercise intensities.
From a psychological perspective, RPE is also related to dispositional and situational factors (Morgan, 1973; Morgan, 1994; Noble & Robertson, 1996). For this reason, it is necessary to understand how RPE correlates with exercise intensity, especially with high intensity. In this context, a more robust understanding of connections and links between physiological (e.g., HR, V̇O2) and psychological (i.e., RPE) parameters, and the transferability of this relationship during steady-state exercise could also lead to increased accuracy of aerobic exercise intensity prescription. Furthermore, Hall, Ekkekakis & Petruzzello (2005) found that the relationship between the factors above becomes weaker as the intensity increases, probably because high exercise intensities are those in which personality and cognitive influences begin to subside.
It is worth noting that the results of the present study were collected in a small and homogenous sample of young, physically active, and healthy males; hence, future studies should assess those relationships in different populations (e.g., females, sedentary or pathological individuals). The lack of a priori sample size calculation and power analysis is due to the fact that the present study is a retrospective analysis using the data collected in the companion article by Ferri Marini et al. (2022a). However, the results reported in the present study (i.e., effect size (Table 3), over- and under- estimation on an individual level (Table 4), and supplementary individual raw data) can provide preliminary information that may help researchers and practitioners to delve deeper on the topic of the transferability of the relations between physiological and psychological exercise intensity indices from incremental to prolonged exercises.
Finally, a limitation of the use of RPE, which is also present in the present study, is that perceived exertion could be affected by the exercise sessions previously performed. However, in the present study, the presence of a systematic bias caused by this issue should be mitigated by the randomization of the experimental trials and the compliance with the standardized anchoring procedures and pre-test instructions used before each experimental trial, which specifically inform the subject to express their perceived exertion without considering the previously reported values (ACSM, 2012; Schoenfeld et al., 2021).
In addition, the results of the present study also suggest that it would be advisable not to rely on only one parameter (i.e., HR, V̇O2, power output, or RPE) to prescribe and monitor aerobic exercise intensity but rather to use a combination of multiple parameters. This approach could help researchers and practitioners to increase the aerobic exercise intensity prescription accuracy and the benefit-to-risk ratio of aerobic training.
Conclusions
This study adds information to its companion article, showing that prolonged exercise duration and intensity could affect not only the relationship between HRR and V̇O2R, but also their relationship with RPE. Indeed, the transferability of the individual relationships between RPE and physiological parameters (i.e., HRR and V̇O2R) found during incremental exercise to prolonged exercise, hence their validity in prescribing aerobic exercise intensity during prolonged aerobic exercise, was not confirmed in the present study. Therefore, to accurately prescribe and monitor aerobic exercise intensity, exercise professionals should be aware of the physiological and psychological adjustments happening during prolonged exercise, and future studies should assess how these adjustments are affected by the parameters (i.e., HR, V̇O2, power output, or RPE) used to prescribe and monitor exercise intensity. Finally, although RPE represents a valuable method to prescribe exercise intensity, it is recommended that the subjects are familiarized with using it and that, for exercise prescription purposes, RPE is used alongside other parameters.